Scoliosis
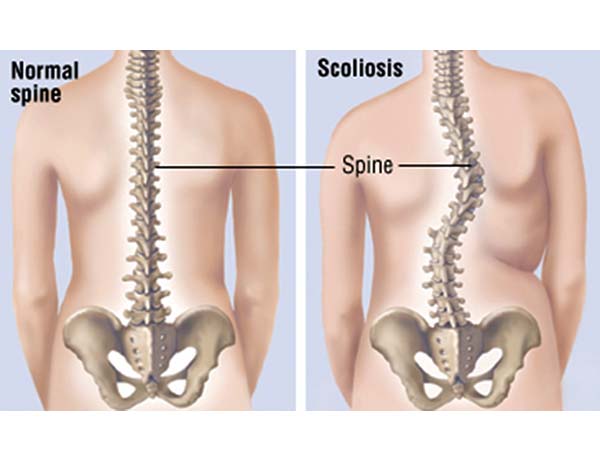
Scoliosis, which is the term used for a spine with an abnormal sideways curvature, which is commonly associated with a rotational abnormality commonly occurs within the growing spine and is more common in females. It affects approximately 2% of the population and can run in families. The normal spine is straight when you look at it from the front and a diagnosis of more than 10º of side curvature is required to make a diagnosis of a scoliosis.Common causes of scoliosis:
1) Idiopathic scoliosis – this occurs either in the younger age group under 10 years of age, which is more uncommon but tends to occur in the adolescent age group between 10-17 years of age. Due to the rotation of the spine then the shoulder blade or the loin can become more prominent and occasionally the shoulders are not level.
2) Neuromuscular scoliosis – this refers to some form of neurological or muscular condition that secondary results in scoliosis. Commonly this can either be cerebral palsy, muscular dystrophy or spinal cord injury. There are several other causes.
3) Congenital scoliosis – this occurs if there has been an abnormality in the growth of the vertebrae and tends to be picked up on an ultrasound scan during pregnancy. The vertebrae can either fail to form properly or can fail to separate which can lead to a scoliosis which will need monitoring after delivery.
4) Degenerative scoliosis – this condition tends to present in the over 40s age group. This can either occur as a new event as the spine goes through a degenerative process or it can be associated with a pre-existing idiopathic scoliosis which has deteriorated.
Many patients can have little or no symptoms from the scoliosis. Others can have uneven cosmetic appearances of the loin, ribs or shoulders. Some can present with pain. This seems to be in 30% of cases. Neurological symptoms are very uncommon in the younger age group. Pain and nerve symptoms are more common in the adult population.
Scoliosis is diagnosed by an Adam’s forward bend test which tends to accentuate the curve. The flexibility of the curve can be assessed by stressing the curve in this position. In a standing position the levels of the pelvis and shoulders are assessed as well as the prominence of the scapular and loin creases also noted. An appropriate neurological examination will also be performed.
Standing standard x-rays are usually performed and this will allow assessment of the degree of the curve and the skeletal maturity, which is important in respect of the risk of progression.
Appropriate treatment for children is dependent on the curve, it’s location and the child’s skeletal maturity. Initially the curve is monitored and occasionally brace therapy instigated. Bracing does not cure the scoliosis but may prevent progression during a growth period. If a curve progresses to more than 40-50º then surgical correction will be considered.
In the adult scoliotic group, management is determined by symptoms in respect of pain and functional limitation. Normally pain is related to the disc, facet joint, sacro-iliac joint and from nerve compression. Therefore, a multidisciplinary management plan is required in the form of medication, injections as well as physical therapy.
Surgery is reserved for patients with poor quality of life and can be either performed from the back, front or a combination of both, be that a 360º fusion. It is important that type of surgery is performed in specialist centres who do this surgery routinely.
Please see more information on procedure for Scoliosis in Children . Please see more information on Paediatric Scoliosis from NUvasive on Paediatric Scoliosis. Please see more information on Adult Degenerative Scoliosis and Possible Treatment Anterior Lumbar Interbody Fusion (ALIF)