Disc Herniation
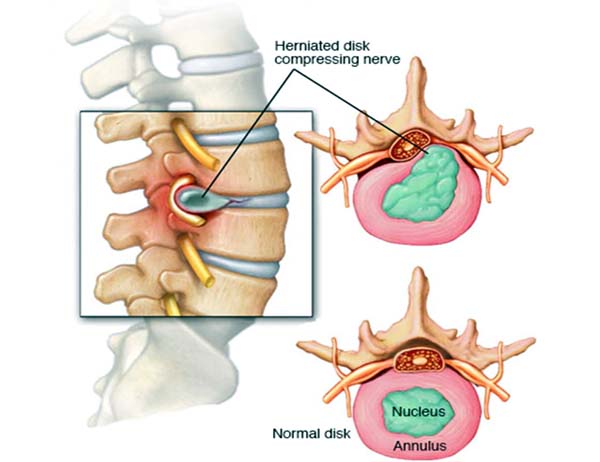
Discs sit in between each vertebrae and act as a shock absorber. Due to varying factures, as we age, the disc goes through a process of dehydration, this makes it stiffer and offers less shock absorbance. The normal disc has an outer fibrous layer, called the annulus and an inner jelly like substance which is called the nucleus pulposus. As the disc goes through degeneration the distinction between the jelly like substance and outer fibrous layer becomes more indistinct. A herniation of the disc occurs when there is a hole in the outer annulus and some of the nucleus extrudes through it. Disc herniations are very common and may not cause any symptoms and this has been shown on MRI scans of normal subjects which becomes more common as we get older. A tear in the outer annulus can result in neck or back pain. If the disc herniation presses against the spinal cord or nerves, then symptoms can result in relation to spinal cord dysfunction or nerve irritation resulting in leg or arm pain, numbness or weakness.Assessment in the clinic will involve an appropriate history and physical examination in the form of a neurological examination to try to identify which nerve has been irritated and to assess its functioning. Specific nerves in the neck and in the lower back supply particular muscles and area of skin and therefore the neurological examination will try to correlate this to the appropriate disc which will be confirmed by the preferred test, which is an MRI scan.
Treatment initially is to exclude associated neurological injury, be that spinal cord compression, bladder/bowel dysfunction or deteriorating neurological functioning to either leg. If this is excluded then initially a conservative management plan would be followed with regards to observation, medication including anti-inflammatories and codeine/paracetamol with physical therapy. If pain is difficult to control, then different neuroleptic medication or a steroid injection called a nerve root block could be utilised to manage symptoms allowing natural history to occur. 75% of nerve related symptoms settle over the first six weeks and up to 90% over the first three months. If symptoms do not improve with conservative management or there is deteriorating nerve function, then surgical decompression to decrease the pressure on the nerve would be considered. Discectomy/decompressive procedures are appropriate to take the disc fragment from the lower back whereas in the neck an anterior approach removes the entire disc which may require replacement with a disc replacement or fusion cage. Disc herniations in the thoracic spine are uncommon and may require an approach from the back or through the side of the chest to remove the disc fragment away from the spinal cord.
It is important to remember that surgery removes the fragment of disc impinging on the nerve, but the majority of the host disc is left untouched. Therefore, there is enough disc remaining to act as a required shock absorber, but this disc is not normal. It is therefore important after surgery to go through a good rehabilitation and strengthening program as the disc can go through further degeneration that may require further treatment. Some patients remain asymptomatic while others can have a recurrence of the disc herniation that requires further treatment which may involve fusion.
Pease see more information on Disc Herniation, diagnosis, treatment and post treatment















